
What is a SLAP tear?
What is a SLAP tear? The term SLAP is an acronym for “Superior Labral tear from anterior to posterior”.
But first we need to understand what a labrum is.
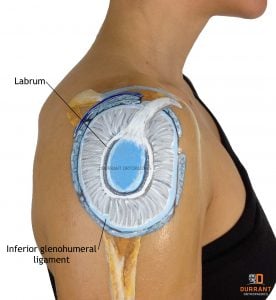
The shoulder labrum is a lining around the socket of your shoulder. It’s a rolled-up structure and it sits on the very rim of the socket.
It deepens the socket and provides a contact area for the humeral head. It also provides attachment points for the ligaments around the shoulder, in particular the inferior glenohumeral ligament, which is the very bottom ligament that runs from the socket to the ball.
Its purpose is essentially to help stabilise the shoulder.
If you were to look at the shoulder socket face on, it is vaguely pear-shaped in appearance.
It is wider and broader at the bottom and it narrows at the top. If you cup your hand, that is essentially the shape of the shoulder socket.
It is not like the hip joint socket that looks more like a tow-bar coupling with a deep socket and large ball that provides a lot of stability.
Your shoulder joint is very unstable but it needs to have that range of movement. If you are going to have a big range of movement and you have an unstable joint, you need to have a way of stabilising it throughout its range of movement.
And that’s where the labrum comes in.
Labrum tears and shoulder instability
When doctors talk about shoulder instability, the labrum is one of the things they go in and try to repair.
By repairing the labrum, it indirectly re-tightens the ligaments and re-attaches all those ligament structures to the shoulder socket.
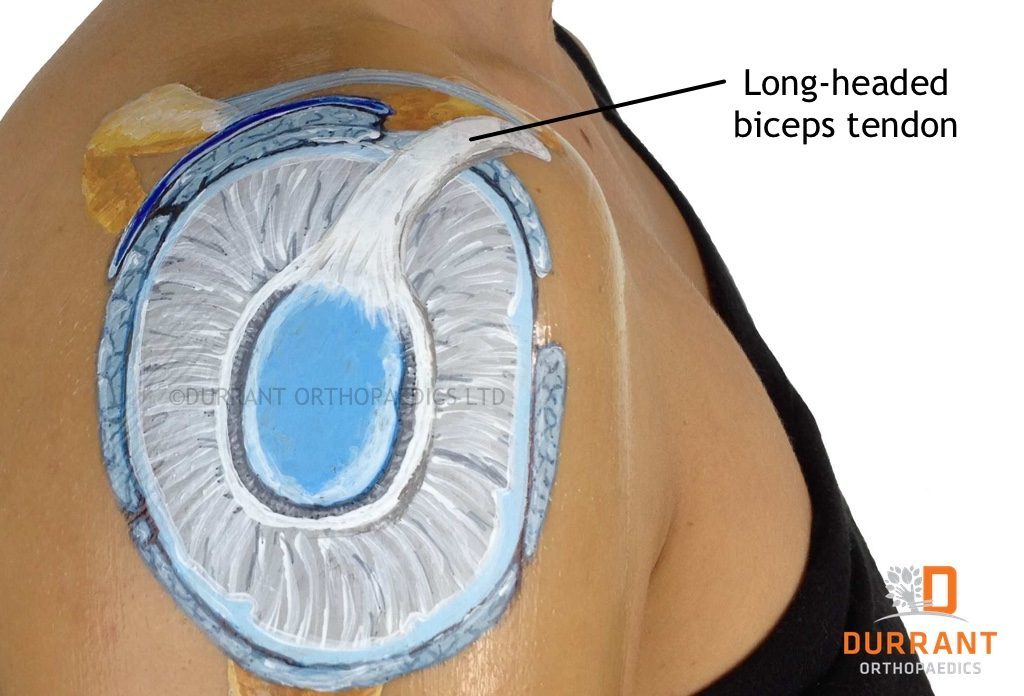
There is also a tendon that runs into the shoulder called the long-headed biceps. It is a muscle that is actually made up of two muscle bellies. Most of it attaches to the spikey bone at the front of the shoulder.
You can feel it if you push hard enough just in front of the clavicle.
The smaller tendon, the long head, runs up through a gap, across the top of the shoulder, and sits in a groove as it runs up the side of the shoulder.
It then attaches to its own little lump of bone at the top of the socket, and indirectly through into the labrum as well.
If you sustain an injury to the long-headed biceps, you can injure the labrum, or, if you injure the labrum, you can end up with symptoms coming from your long-headed biceps.
What is a SLAP tear?

SLAP tears were first described in North America by athletes who did repetitive overhead throwing.
Athletes such as baseball pitchers or quarterbacks were susceptible due to repetitively throwing overhead.
It is a result of what is called a “roll-back phenomenon,” where the shoulder constantly comes upwards and into contact with the top of the labrum and eventually just scuffs it off with this repetitive overhead throwing action.
It is also a deceleration injury because your biceps tendon and muscle are actually contracting as your elbow is extending to throw, trying to decelerate and control it.
Hence, in these pitchers who are throwing at high velocities and putting huge stresses on their elbows, their biceps are important in decelerating their elbow to try and prevent it from injuring itself.
However, that puts pressure through the biceps tendon and up inside the shoulder.
People started to complain of superior shoulder pain, particularly when throwing, and they would often get a ”dead arm” feeling when they tried to throw.
They would sometimes experience clicking or catching from within the shoulder.
This is a mechanical symptom – it’s a tear, a piece of tissue that can flick over and lay on the shoulder.
When they brought their shoulder up and into that pitching position, they were catching on it, riding over it, which gave them pain.
It also gave them the mechanical symptoms of that click or catch feeling in the shoulder.

What injuries cause SLAP tears?
There are two types of injuries that cause SLAP tears – there is the non-traumatic or degenerative change, which is predominately in the throwing athletes.
That can be part of a spectrum of injuries called internal impingement, where there is also damage to the rotator cuff at the same time.
This is because the person has an extreme external rotation, which is the ability to roll the shoulder back to create a nice, big, strong pitch.
They actually start to crimp the back of the rotator cuff against the socket as well, so they damage their labrum and their rotator cuff.
The other type of tear is traumatic, which is the type that is most common here in New Zealand.
This type of tear tends to be as a result of falls or a pattern very similar to that, which would lead to dislocation.
In a dislocation, the arm is brought back into the externally rotated position, like in a rugby tackle, and the shoulder gets pushed out to the front of the joint.
Doctors are not 100% sure about the nature of how these traumatic lesions occur, but the broad categories are a push-off or a pull-off lesion.
A push-off lesion is when the humeral head (the ball) has ridden up and pushed the labrum off or scuffed it back up and off.
A pull-off lesion, or a traction lesion, is when you grab hold of something and your arm is pulled out and away from your body, pulling on the long-headed biceps, which then pulls the labrum away.
There are many theories about which is which, and it’s difficult to prove.
Are there different types of SLAP tears?
There are different grades of tears; they range from tears that just involve the labrum, to tears that involve the biceps tendon.
It has a little horizontal portion, which is the bit that runs across the shoulder. So the tear can actually split up into that and flaps of tissue can actually come off the biceps tendon as well.
The type of tear determines the type of repair that can be done. This is also dependent upon the age of the patient.
The grading system began very simply, using numbers one to five. Now it has gone beyond that and it is quite complex.
It is difficult to predict the grade of a tear, depending upon the injury, and realistically it’s also hard to predict the treatment unless you are at the very extremes of those grades.
An MRI is not particularly good at picking up the grade of a tear – it can give an indication, but arthroscopic surgery is the time where a grade can formally be given.
With the difficulty in diagnosing a SLAP tear, the gold standard is an MR arthrogram, which relies on the dye tracking up under the labrum.
What are the treatment options for SLAP tears?
The first step in treatment would be rehabilitation.
This would involve going through a period of trying to strengthen the shoulder, trying to control the kinetics, or movement, of the shoulder to try and modify what actions they are doing.
If it is an older person, they may decide that instead of going down an operative pathway to get back to sport, it might be time to hang up the boots.
If physical therapy is not working, then that’s when you seek a surgical opinion, usually provided by either a sports orthopaedic or shoulder orthopaedic surgeon.
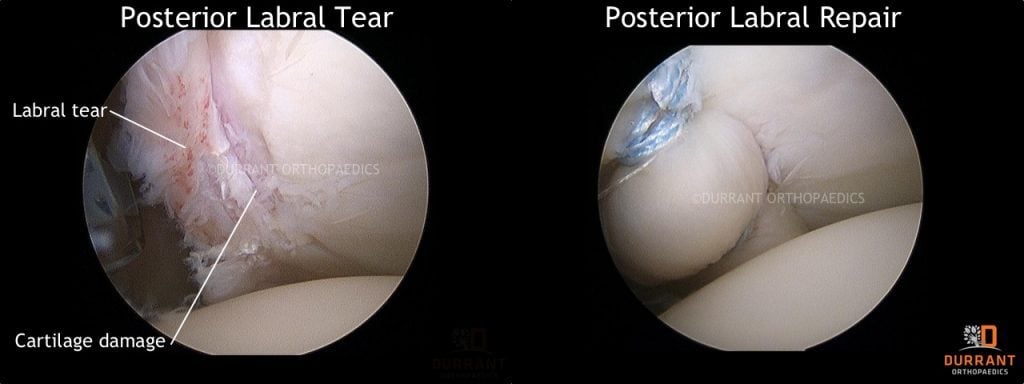
This could involve trying to deal with all the instabilities, aiming to try and re-attach the biceps tendon to the top of the socket by repairing the superior labrum, cleaning and freshening it up, and reattaching the labrum using anchors.
Doctors will obviously also deal with any other pathology they find in the shoulder at the same time.
If it is an older person or a contact athlete, sometimes a biceps tenodesis is a more reliable option than a superior labral repair. A superior labral repair can sometimes lead to a bit of shoulder tightness, so the biceps tenodesis is often a better option, particularly in this particular group.
What if I need surgery for a SLAP tear?
Doctors will arthroscopically remove the tendon from the superior labrum, then reroute the tendon back into the outside of the shoulder and reattach it at the front of the shoulder.
This shortens the attachment by a couple of centimeters, but the tendon continues to function normally.
The advantage of doing a shoulder stabilisation arthroscopically is that it can be done through small incisions. However, sometimes doctors have to convert the arthroscopic approach to an open approach if they are having trouble seeing.
The tendon is reattached with a screw, by drilling a small hole, placing the tendon into the hole and then running the screw over the top of the tendon into that hole. The screw is often slightly larger than the hole and the tendon to provide a tight, compression fit.

What can I expect after Labrum surgery?
SLAP tear operations are normally done as day operations. Your dressings will be changed the following morning, your anaesthetist will give you pain relief and you’ll usually have a numb arm for the first 12 to 24 hours.
After that, you are in a sling for four weeks.
You will receive simple exercises to do to keep the shoulder mobile, but not put any undue stress on the repair, and at the 4- to 6-week mark, you start to see a physiotherapist who will progress you through rehabilitation.
In most cases, rehabilitation is done in six-week blocks.
The first six weeks is passive movement, or using the shoulder with the assistance of gravity, or with gravity eliminated, not putting any load on it.
Then for the next six weeks it is using your arm normally, but without any load, so you are not lifting or carrying anything with that arm, and then finally at the twelve-week mark you start doing some strengthening.
When can I return to work following a SLAP tear?
If you are a desk-bound worker, you could be back at work within 48 hours of your procedure if you really wanted to be, but if you are a heavy, manual labourer, a builder, something that involves overhead activities, you are still possibly looking at between four and a half to five months before you can return to normal overhead activities.
You could, however, be back to doing most activities below or at shoulder height a little bit earlier than that.
While it is possible to re-tear; however, the chances are low.
If you are experiencing any of the symptoms mentioned in this guide please contact Mr Durrants clinic on (09) 523 2765 for more information. If you are in pain from a recent injury please seek immediate medical attention from your nearest accident and emergency clinic.