
AC Joint Seperations
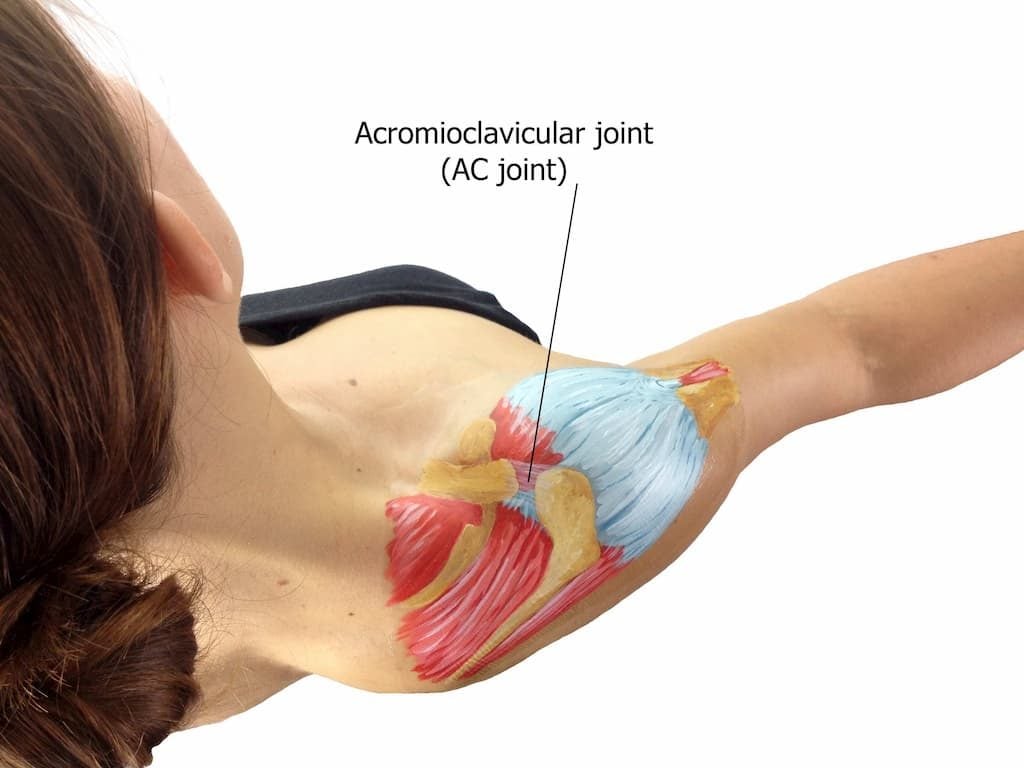
Your AC joint can be found in your shoulder, at the outer end of the collar bone (the clavicle) and the top of your shoulder blade. The purpose of the AC joint is to suspend your shoulder off from the clavicle.
It often feels like a small bump at the very end of your clavicle.
The AC joint has very little movement in it; it can only rotate between 10 and 15 degrees at most, and this decreases with age. By the time you are 40, your AC joint will have very little movement in it at all.
The joint allows you to be able to move your shoulder up to the front and out to the back. It also helps with the rotation of the shoulder, mainly moving your arm in or out.
What are AC joint injuries?
The most common injury I see to the AC joint is arthritis and this is where the bone wears out. It is very common in people over the age of 40 to have some form of arthritic change in their AC joint from natural wear and tear over time.
People who are body builders or those who do a lot of heavy lifting can suffer from post-traumatic osteolysis of the outer end of the clavicle, which is softening of the bone.
How are AC joint injuries classified?
Your AC joint is susceptible to a wide range of injuries, but the most common is an AC joint separation or dislocation.
How it is referred to depends on whether it is based on American or British literature.
AC joint injury is often called an AC joint separation, but the word “dislocation” is used interchangeably, so in New Zealand it would be an AC joint dislocation, but in America they call it an AC joint separation.
Are AC joint seperations different to shoulder dislocations?
It is essentially the same type of injury.
This injury can range from a very mild sprain all the way to a complete dislocation of the joint. The patient’s dislocation is diagnosed based upon a grading system.

This system was designed by several surgeons over time, but most recently has been modified again into six grades that vary in intensity as they increase.
What about traumatic AC joint injuries?
Unfortunately, AC joint injuries are not preventable. Traumatic AC joint seperations are most common in contact athletes and cyclists.
This is when there is a blow to the outer end of the shoulder, the arm is across the front of the body and the shoulder gets pushed down while the clavicle stays up.
So in an AC joint seperation, your clavicle actually hasn’t gone up, even though that’s what it looks like. Instead, your whole shoulder has come down and forward.
For a rugby player, that type of injury would most commonly come from a shoulder charge or tackle.
For a cyclist, it’s when they are thrown over the handle bars and land on the back corner of their shoulder as they roll over, or if they are hit by a car and go up onto the bonnet.
Very occasionally it can be as a result of a defend-type injury, where you have put your hand out and the shoulder just gets physically pushed back, but that’s very uncommon.
Other cases include multi-trauma injuries such as high falls and car accidents.

What does it feel like?
A mild AC joint injury can often be misdiagnosed as a sprain that just has some pain that eventually goes away over time.
However, significant injuries are very painful, and usually have a deformity, a noticeable lump or step at the end of the clavicle.
There is often a feeling of pain where that deformity is, but this pain can radiate down into the front of the shoulder and occasionally up into the neck.
The pain usually intensifies if an attempt is made to bring the arm across the body, as if you were trying to put on a seat belt.
When should I see a doctor?
If you think you have an AC joint injury, it is beneficial to see a doctor straight away to confirm it is a dislocation and not a fracture, sprain or other type of injury.
This will first be determined by physical examination performed by an orthopaedic specialist.
Key identification markers of an AC joint seperation include pain in the area and a step or instability of the outer end of the clavicle – you can push on it and it goes down like a piano key, or you can push on it and it reduces.
It will also reduce if you push up on the elbow because you are pushing the entire shoulder joint back up onto the AC joint.
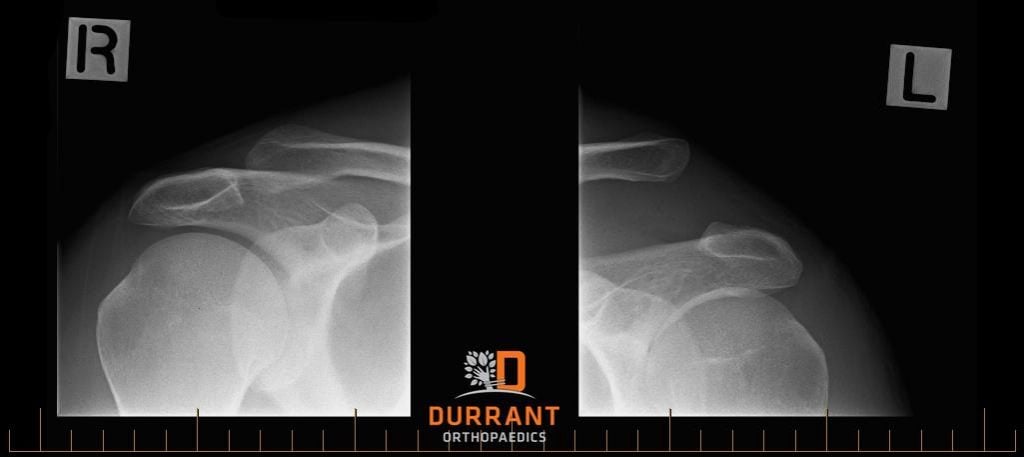
In addition to a physical examination, an x-ray is usually performed to identify an AC joint injury.

The x-ray will include a direct, front-on view with the beam tilted slightly to look up through the AC joint more accurately. Sometimes a weight bearing x-ray is taken, where you hold a weight in that hand to try and accentuate the degree of the deformity.
An x-ray will then be performed on your other shoulder for comparison, as everybody’s AC joint is slightly different.
Do all injuries require surgery?
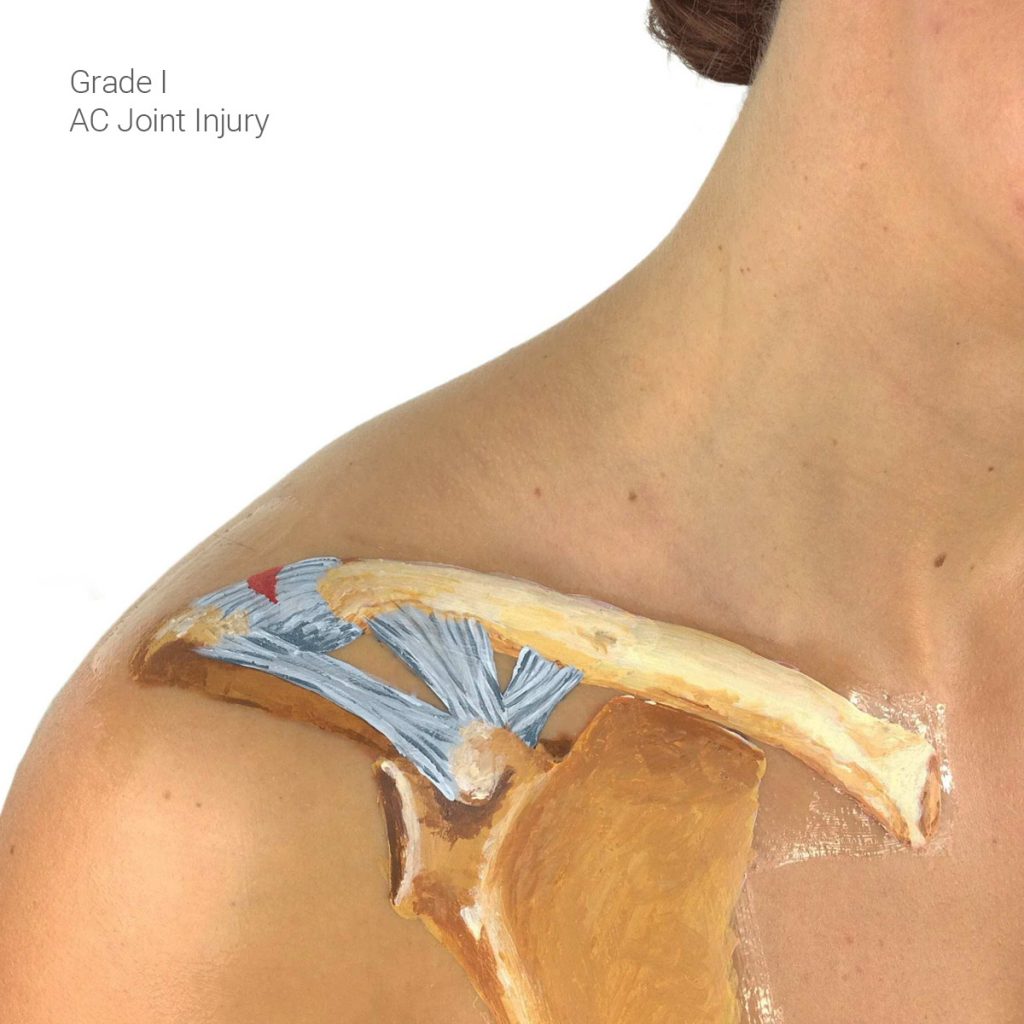
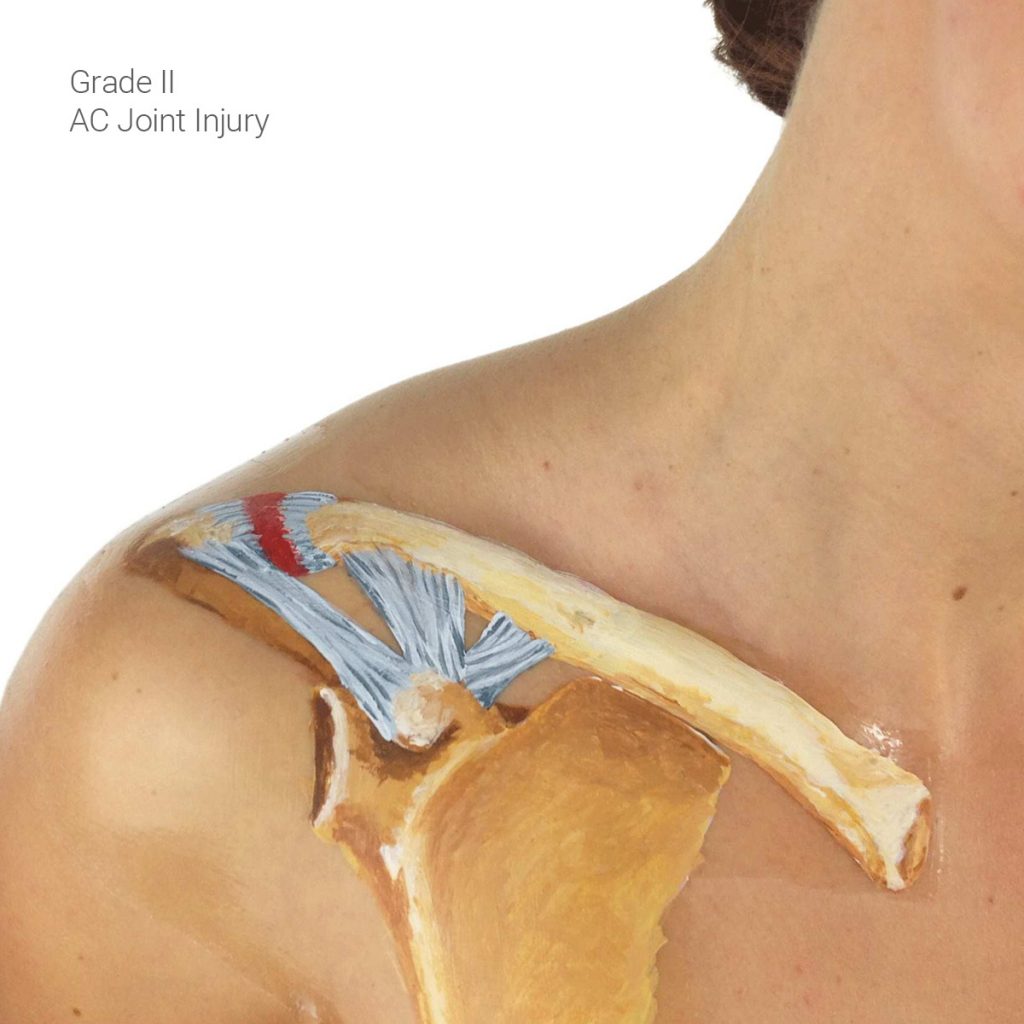
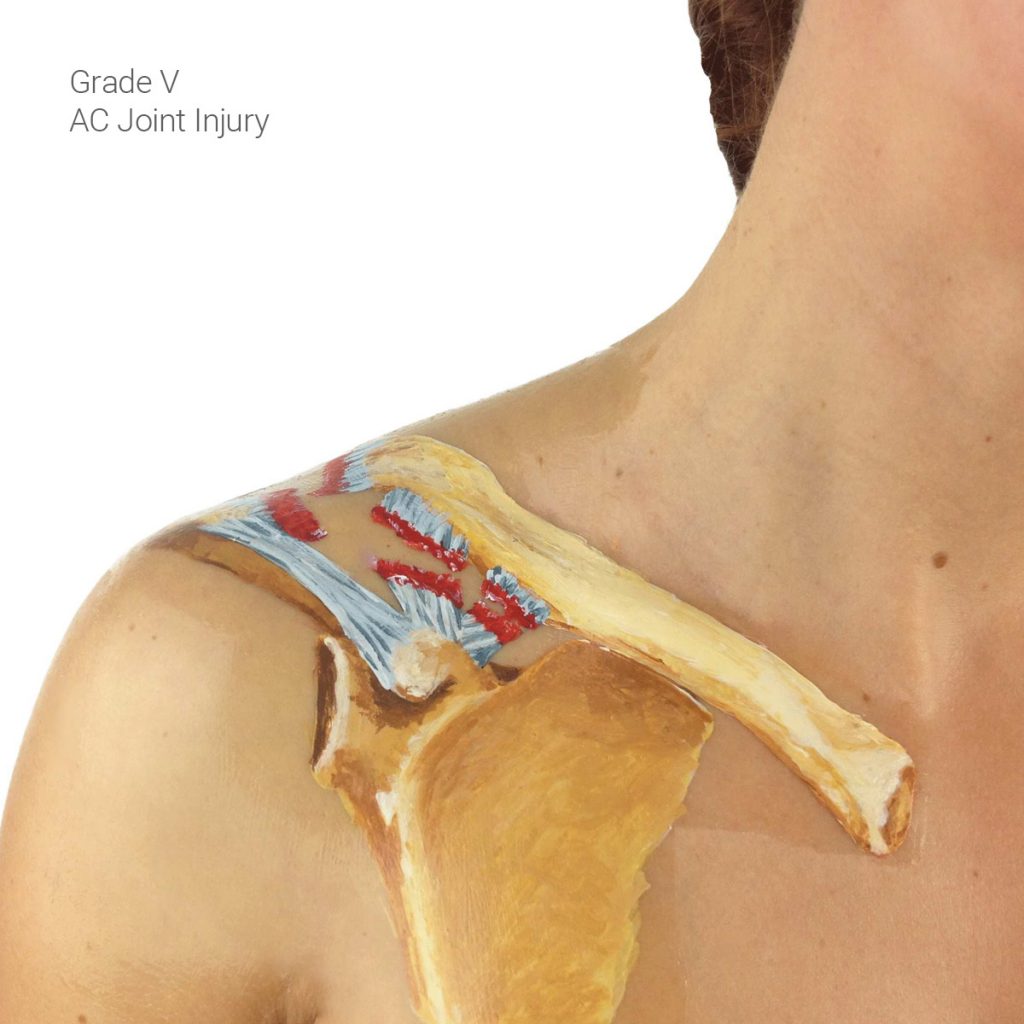
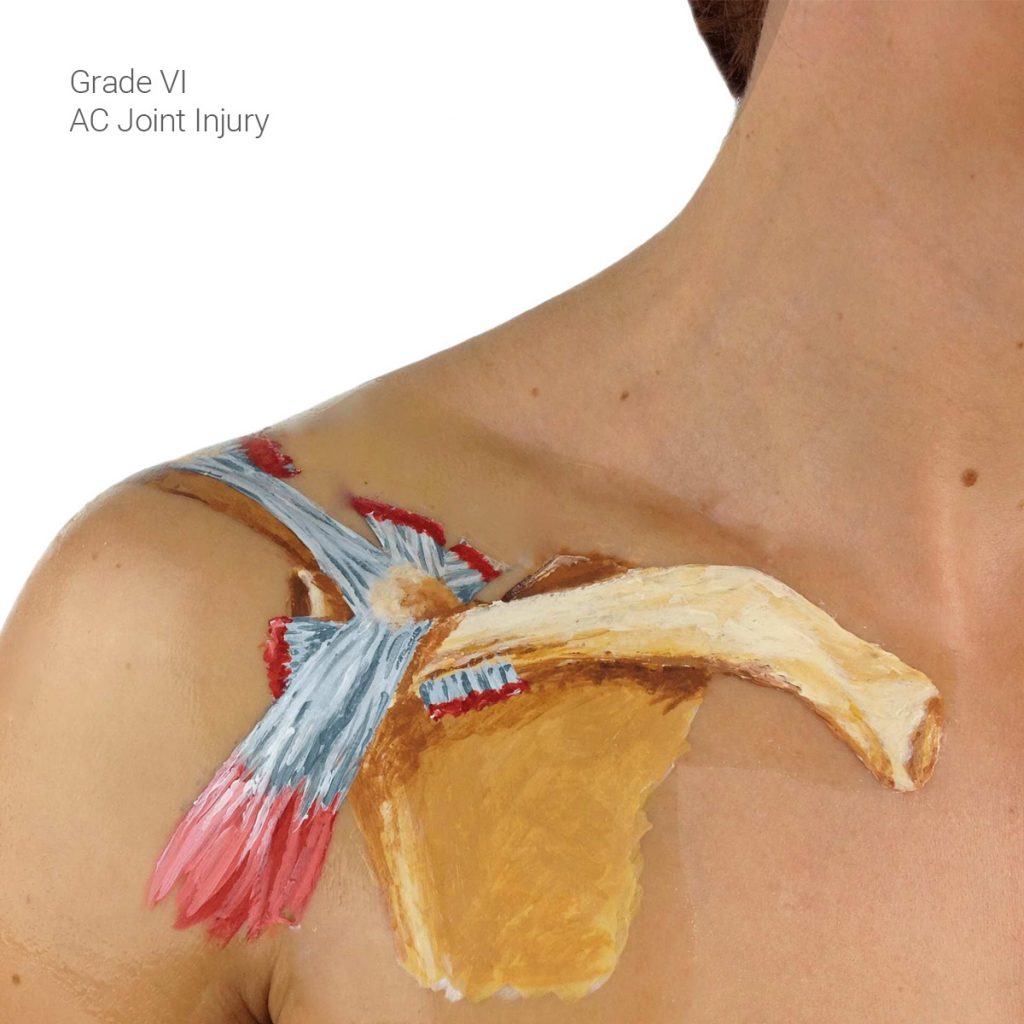
If you do have an AC injury, it will be classified into one of the six grades to select the appropriate treatment.
If the AC injury is of the lower grades, often I or II, the treatment process doesn’t require an operation.
Grades IV, V and VI will require an operation for effective treatment.
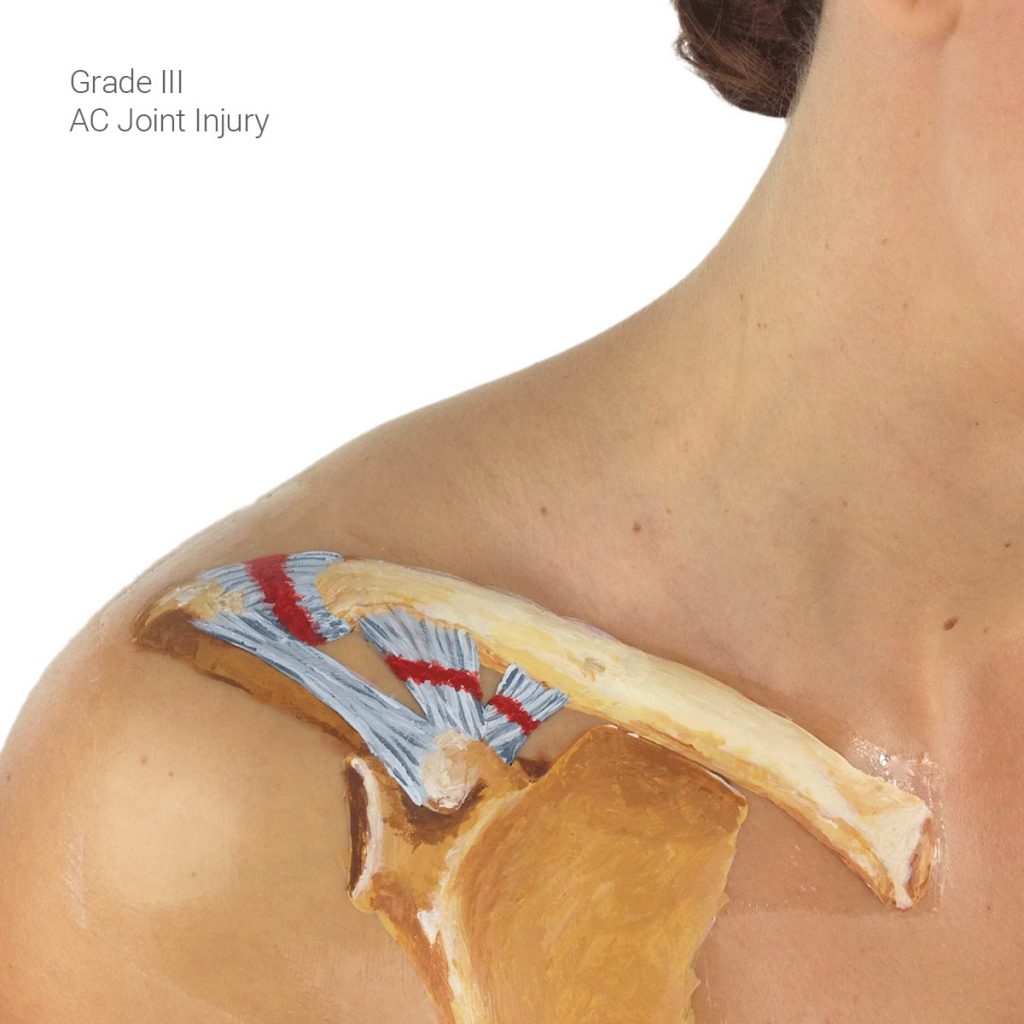
Treatment of a Grade III AC joint injury, where the joint has separated and subluxed slightly and is partially dislocated, is controversial, and is really decided on a case-by-case basis as to whether the injury should be operated on or not.
Some people advocate early treatment, some people advocate leaving it for a while.
For a Grade III injury, it is best to see an orthopaedic surgeon for their opinion.
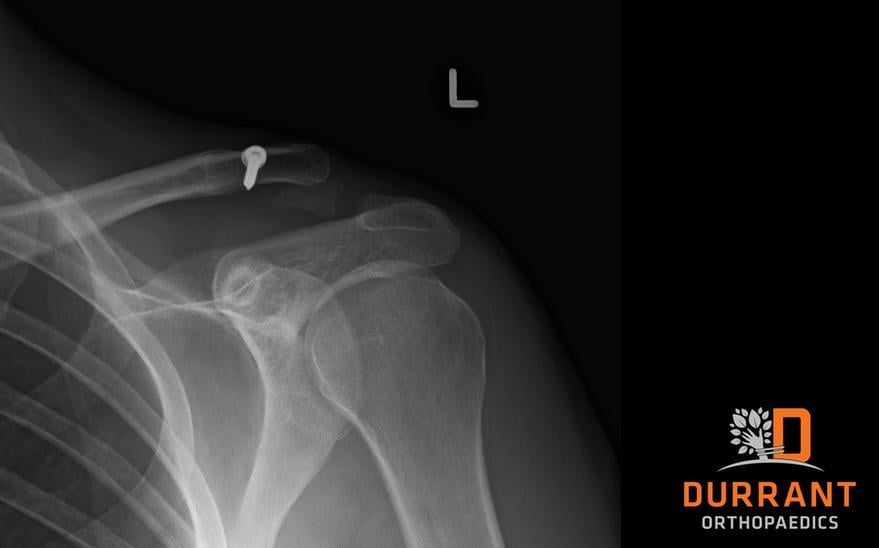
What is involved with surgery?
If surgery is required, the procedure is done by keyhole, (a minimally invasive procedure using very small incisions).
It is usually successful if the joint is reduced and operated on within the first two weeks after the injury, but after that the success rate drops off.
At that point , surgery becomes an open procedure, which is designed to reconstruct the ligaments of the shoulder to allow them to heal and be replaced.
There are two main types of surgical procedures. One uses an artificial ligament, which is designed to pull the clavicle down and back into its normal position.
The other type of operation is to try and reconstruct the ligaments, using a hamstring, either from the patient’s knee or from a cadaver (called an allograft hamstring), The choice of operation usually depends upon the patient’s wishes.
Using an artificial ligament can have potential complications with the devices used to fix the artificial ligament in place.
However, there is no need to operate on the patient’s knee to acquire the hamstring, and the artificial ligament is much stronger, which allows for a quicker rehabilitation and recovery process.
One main shortcoming to using the hamstring to reconstruct the AC joint is the requirement of a secondary procedure to acquire the ligament from the patient’s knee. This does run the risk of causing problems of immobility for the patient.
With this type of surgery, you will also need to have your arm in a sling for a longer period of time and rehab is slower because more time is needed to allow for the growth of tissue around the ligament to make it stronger.
The same risks exist for both procedures such as re-dislocation, failure of the ligament reconstruction, infections and nerve damage.
What happens after surgery?
After the procedure, you are usually kept in hospital for a night, and before leaving, a physiotherapist will see you and give you small, simple exercises to complete at home.
Your arm will also be in a sling for 4 to 6 weeks.
Approximately two weeks after the surgery the stiches will be removed, and at the end of the six weeks the rehabilitation will begin, including active movement exercises. This is when you start moving your shoulder using your own muscles.
After that, you will begin a strengthening exercise program that is outlined and directed by a physiotherapist.
When can I return to work and sports?
If your work is sedentary, such as sitting at a desk writing and typing, you could expect to be back at work within 1 to 2 weeks.
However, if you are an overhead, manual worker, it will probably be closer to 3 to 4 months before you can return to active duties in your job.
Furthermore, for a contact athlete like a rugby player or basketball player, they won’t be able to return to playing for at least 5 to 6 months.
Can arthritis and “stiff shoulder” become an issue?
There are some risks post-surgery, one being that your shoulder could become permanently stiff.
However, this is uncommon, with only 1 to 3 percent of operations resulting in this outcome.
There is also a risk of arthritis developing in the AC joint in the future, but this can also occur in people who have never had and AC joint injury.
During surgery, a little piece of the clavicle is cut off to unload the AC joint to prevent the chance of arthritis developing in the future.
There is no reason why an athlete can’t return to playing contact sports and lifting weights after an AC joint injury or surgery.
Can surgery fail?
One of the main reasons the surgery fails is because the patient doesn’t complete the rehabilitation exercises properly or for the required time.
When it comes to contact athletes, their surgeries fail because they go back to playing too quickly and load their shoulder in exactly the same way again.
The more modern reconstructive techniques are designed around replacing the ligaments with a strong structure, but it is still very reliant on the patient’s body to heal with their own strong tissue and muscle.
If a patient doesn’t take the time to heal, or their tissue doesn’t grow properly, then the implant will eventually fail.
This is more common in the heavy manual worker and contact athlete than it is in the sedentary worker.